Free download: Top 10 Natural & Easy Remedies for Joint Pain from Home. Learn these helpful remedies.
Estimated Reading Time: 12 minutes read
Do you ever get hip pain and wonder what might be causing it? In times like this you may wish you knew more about hip anatomy!
The goal of this article is to give you a basic crash course in hip anatomy 101.
Learn the essentials about the anatomy of the hip in order to better understand pain and where it might be coming from.
Table of Contents
What is the Hip Joint?
The hip joint is also known as a ball and socket joint. It’s formed from the acetabulum of the pelvis and the femoral head, which is the top portion of the thigh bone, or femur.
Not only is this considered a ball and socket joint, but it’s also categorized as a synovial joint. Since it’s classified as a synovial joint, the hip demonstrates the following:
- It has a synovial membrane that releases synovial fluid.
- It has a joint cavity for the synovial fluid to release into.
- The joint capsule is covered with articular cartilage.
- It has outer capsular ligaments that surround the joint.
The hip is a very flexible joint, capable of moving in the following directions:
- Flexion
- Extension
- Abduction
- Adduction
- Internal rotation
- External rotation
Without the support and structure of the hip, we wouldn’t be able to walk, run, sit, squat, climb stairs, etc.
Bony Structures
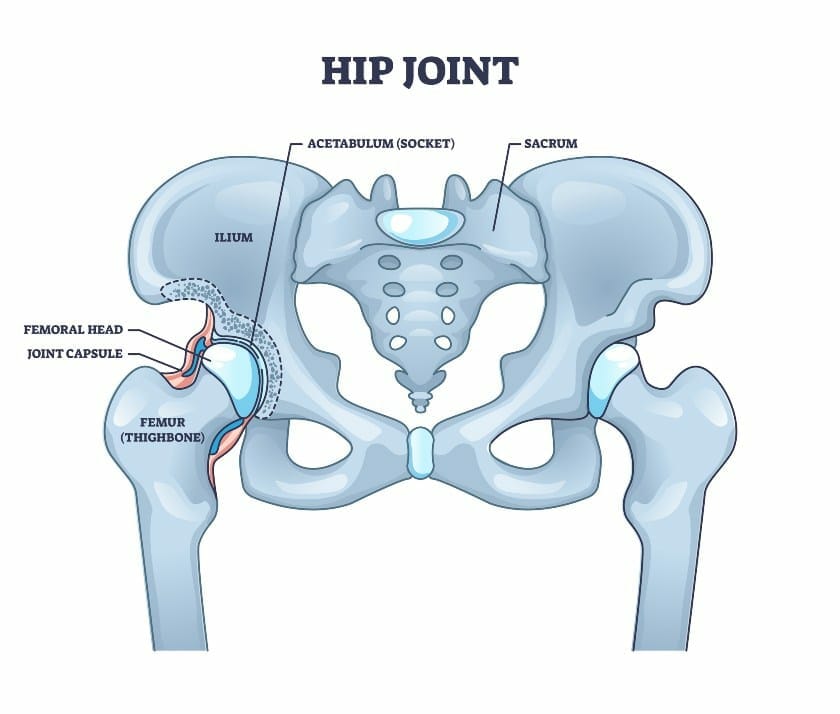
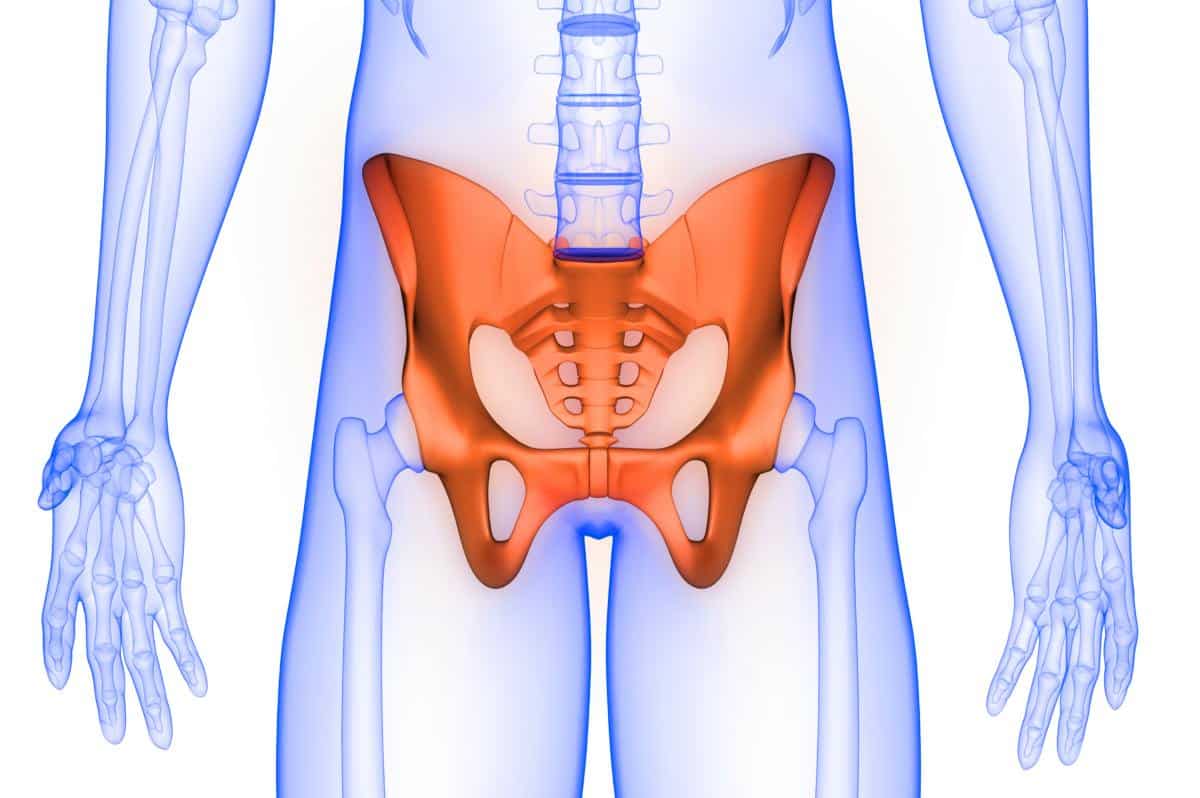
As mentioned above, the hip joint is comprised of components from the pelvis and femur.
The pelvis has a concave region called the acetabulum. The rounded femoral head fits into the acetabulum to form the ball and socket relationship.
The femoral head is connected to the rest of the femur, or thigh bone, via the femoral neck.
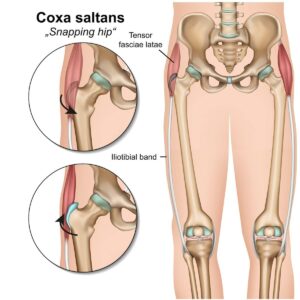
There are also two bony protuberances on the proximal end of the femur called the greater trochanter and lesser trochanter. Multiple muscle and ligament attachments will connect to the greater trochanter and lesser trochanter, which further helps to stabilize the hip joint.
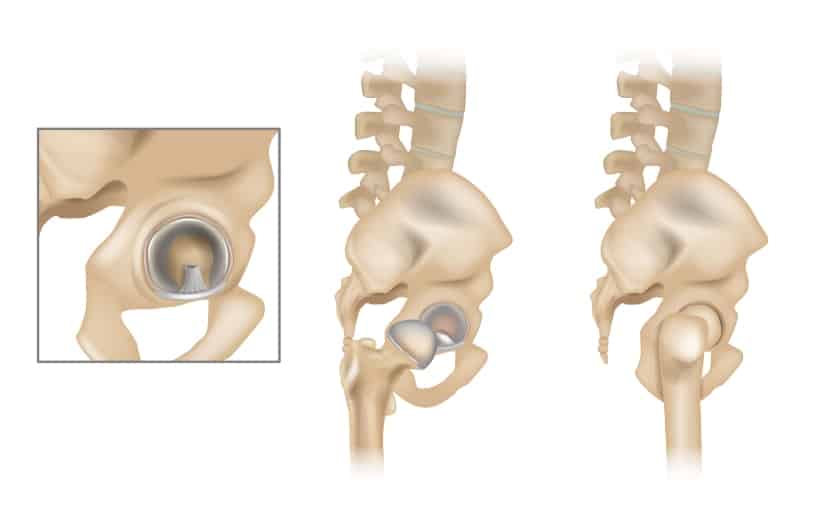
Hip Cartilage
Similar to other joints in the body, the hip joint (both the ball and socket) is lined with cartilage.
The purpose of cartilage is to provide shock absorption during weight bearing activities. It also helps to reduce friction forces as the ball glides in the socket joint.

Advanced hip arthritis and/or direct injury to the cartilage typically leads to abnormal and rough hip joint mobility, which can cause pain when moving.
Synovial Fluid
Synovial fluid is secreted from the synovial membrane in the hip joint capsule. Synovial fluid allows for joint lubrication to ensure a smooth, friction-less gliding motion of the hip.
This fluid will also help to protect the joint cartilage and prevent it from getting worn down so easily. Additionally, regular movement of synovial fluid will allow healthy nutrients into the hip joint.
Regular movement will actually stimulate the creation of synovial fluid. That’s why they say motion is lotion!
Inflammation, or synovitis, within the synovial membrane can lead to hip joint pain, decreased joint mobility and wear and tear of the joint.

Hip Labrum
The hip labrum is fibrocartilage that lines the acetabulum, or hip socket portion of the hip joint.
The acetabular labrum contributes to stabilizing the hip joint by creating a suction-like effect of the head of the femur into the acetabulum. It does this by deepening the acetabular concavity, which will increase the surface area of the acetabulum.
The blood vessels that supply the acetabular labrum include the obturator artery, superior and inferior gluteal arteries.
A proper functioning acetabular labrum will allow full, smooth hip mobility and range of motion. It will also ensure normal alignment of the femoral head in the acetabular socket and will prevent the synovial fluid from leaving the joint capsule.
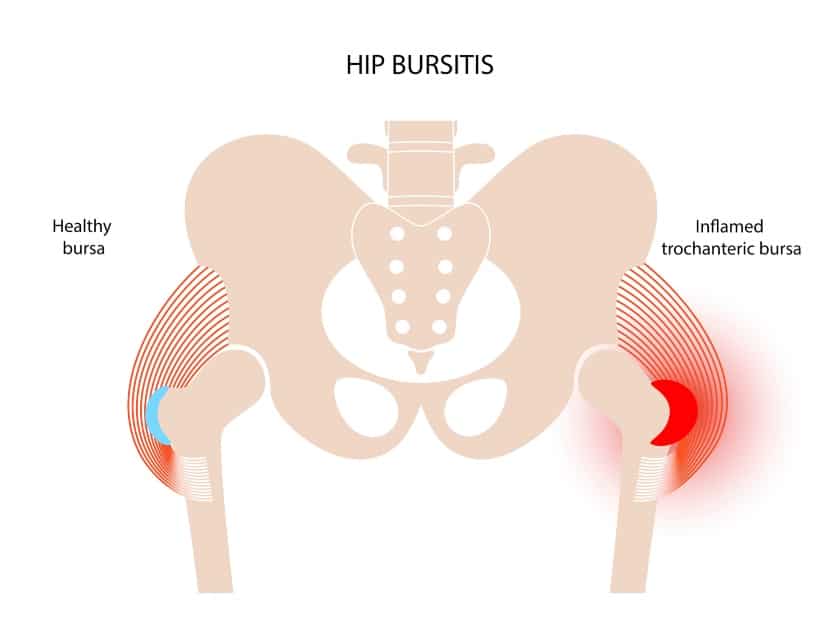
Hip Bursae
Many bursae are found around various joints in the body, including the hip joint. Bursae are fluid-filled sacs that provide additional cushion and support between bones and their attaching soft tissues.
There are two primary hip bursae:
- Iliopsoas bursa
- Greater trochanteric bursa
The iliopsoas bursa lies on the inner thigh or groin near the iliopsoas muscle. We’ll talk more about the iliopsoas muscle in a bit.
The greater trochanteric bursa is located over the greater trochanter. Recall that the greater trochanter is a bony prominence located on the outer edge of the proximal femur.
Inflammation of the bursae sacs commonly leads to a condition called bursitis, which can lead to pain and movement limitations around the hip joint.
Important Hip Ligaments

Ligaments connect bones together. This provides additional support and stability around the hip joint.
There are 4 important ligaments that surround the hip joint that we’ll be discussing. Three of these are located outside the hip joint capsule, while the last is located within the hip joint capsule.
1. Iliofemoral Ligament
The iliofemoral ligament is also known as the Y ligament, with medial and lateral portions to it. This is considered the strongest ligament in the body.
It’s located on the outside of the joint capsule, in the front of the hip, connecting from the ilium bone on the pelvis to a part of the femur called the intertrochanteric line.
The role of the iliofemoral ligament is to limit hip extension, external rotation when in full hip flexion, and external rotation and internal rotation when in full hip extension. It also helps to prevent abnormal pelvic alignment, particularly an excessive posterior pelvic tilt.
2. Pubofemoral Ligament
The pubofemoral ligament is another ligament located on the outside of the hip joint capsule.
It is positioned anteroinferiorly and supports these areas of the joint capsule. It’s located on the pubic bone and connects to the intertrochanteric line as well, blending in with fibers from the iliofemoral ligament.
The pubofemoral ligament limits excessive hip abduction and external rotation when in hip extension. The medial and lateral portions of the iliofemoral ligament contribute to this as well.
3. Ischiofemoral Ligament
The ischiofemoral ligament is considered the weakest out of the ligaments located on the outside of the joint capsule.
This ligament supports the back, or posterior, aspect of the hip joint capsule.
It connects from the ischium to the greater trochanter, below the iliofemoral ligament.
The role of the ischiofemoral ligament is to limit internal rotation in both hip flexion and extension. It helps to ensure the femoral head remains stable and secure in the acetabulum.
4. Ligamentum Teres
The ligamentum teres is located inside the joint capsule. It connects the femoral head to the acetabular notch.
This ligament doesn’t contribute as much towards hip stability as the other above-mentioned ligaments. What it does assist with is rotational stabilization in all directions of the hip, but especially when the hip is flexed greater than 90 degrees.
When taut, the ligamentum teres will secure the femoral head into the acetabulum when the hip is at its end range of motion. This further encourages maximal stability in the hip.
Essential Hip Muscles and Tendons
There are A LOT of muscular and tendon attachments at the hip.
To help make things easier to visualize, we’ll break down and discuss each essential muscle based on its role and action at the hip.
Keep in mind that each muscle has a tendinous attachment that connects it to corresponding bony structures.
1. Hip Flexors
The following are muscles that flex, or bend, the hip. They include the primary hip flexors and other muscles that play a smaller role but still assist in hip flexion.
Primary Hip Flexors:
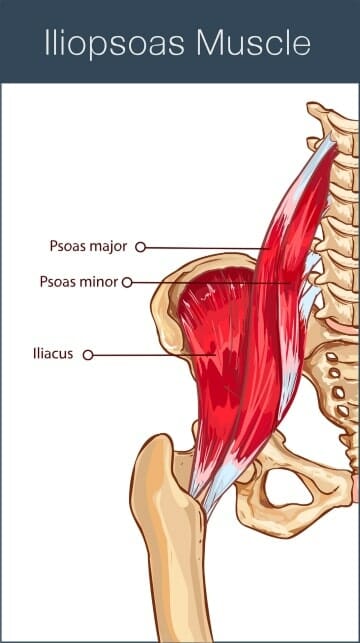
- Psoas major (part of iliopsoas)
- Iliacus (part of iliopsoas)
Secondary Hip Flexors:
- Rectus femoris
- Sartorius
- Pectineus
- Tensor fascia latae
- Gracilis
- Adductor magnus (adductor portion)
- Adductor longus
- Adductor brevis
- Gluteus minimus (may assist in hip flexion)
- Gluteus medius (anterior fibers) (may assist in hip flexion)
The hip flexors are incredibly important for activities such as taking a step forward, climbing up stairs, or stepping over a fallen item on the floor.
The iliopsoas is important for helping to stabilize your posture, including lumbar and pelvic alignment, when in standing.
The secondary hip flexors really are just as important as the primary hip flexors, however, the secondary hip flexors also play a role in other hip and/or knee motions.
2. Hip Extensors
The hip extensors allow you to kick the leg back (as if you’re about to kick a soccer ball), assist in walking with a normal gait, lifting you up onto a step or each stair you climb, and standing up from a chair.
The following are muscles that extend the hip, or the motion of kicking your leg behind you.
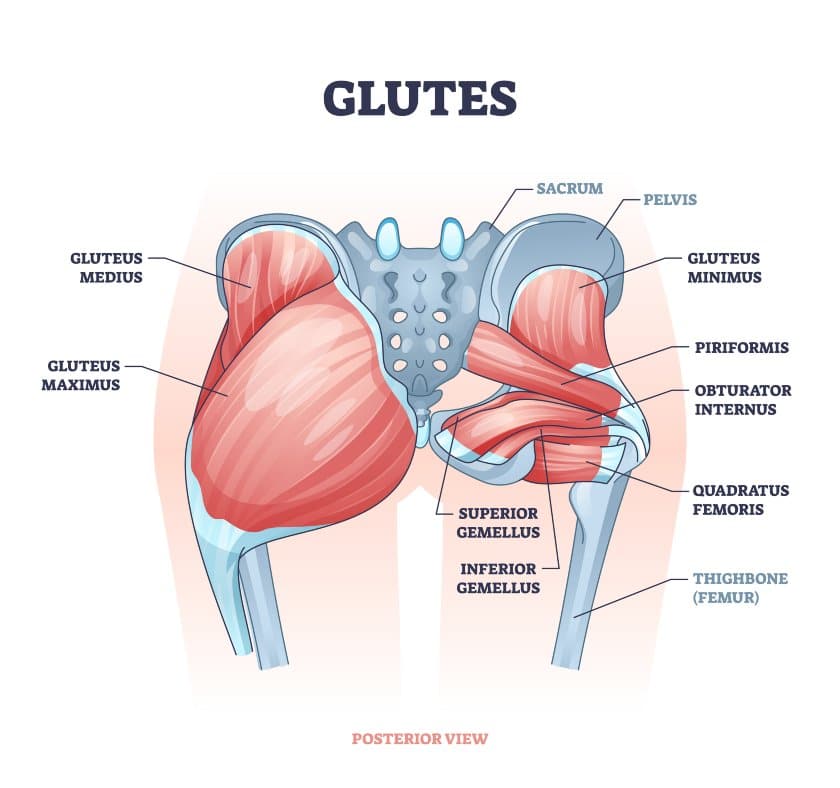
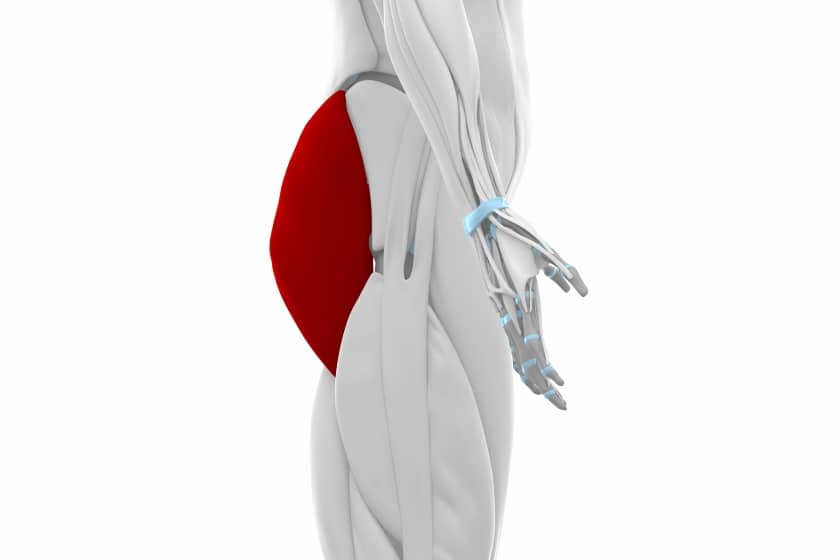
- Gluteus maximus
- Gluteus medius (posterior fibers)
- Hamstring muscles: biceps femoris (long head), semitendinosus, semimembranosus
- Adductor magnus (hamstring portion)
- Piriformis (may assist in hip extension)
Weakness in any or all of the above muscles will make the previously mentioned tasks very difficult and can contribute to hip pain, as well as secondary back or knee pain.
3. Hip Abductors
The following muscles perform hip abduction, or the motion of kicking your leg out to the side or directly away from the midline of the body.
The hip abductors are extremely important for stabilizing the hip. This is necessary for balance, pelvic and hip stability with many of our normal activities and functions.
Primary Hip Abductors:
- Gluteus medius
- Gluteus minimus
Secondary Hip Abductors:
- Gluteus maximus (superior fibers)
- Piriformis
- Sartorius
- Tensor fascia latae
- Obturator internus (abducts the hip when it is flexed)
- Iliopsoas
- Gemellus inferior (abducts the hip when it is flexed)
- Gemellus superior (abducts the hip when it is flexed)
Weakness in these muscles can commonly contribute to low back, hip and knee pain.
If someone has weak hip abductors, they may demonstrate what is known as a hip Trendelenburg. A Trendelenburg is diagnosed when someone is observed to lack the ability to hold the hip in a neutral position when balancing on one leg. The individual will be observed to sink into the hip.
4. Hip Adductors
Hip adductors are responsible for moving the leg directly inward towards the midline of the body. This is a necessary motion to be able to do if you try to cross your legs while sitting.
The following muscles are considered hip adductors, located on the inside of the thigh:
- Adductor longus
- Adductor magnus
- Adductor brevis
- Gracilis
- Pectineus
- Obturator externus (may assist in hip adduction)
- Gluteus maximus (inferior fibers)
Like all of the other hip muscles we’ve discussed so far, the hip adductors help in providing support and stability at the hip and pelvis with standing and walking activities.
5. Hip External Rotators
Hip external rotation is a motion that occurs when the knee and thigh rotate away from the midline of the body. Picture as if you’re kicking the foot and leg up to toss a hacky sack or kick around a soccer ball.
The following muscles are considered hip external rotators:
- Iliopsoas
- Sartorius
- Piriformis
- Quadratus femoris
- Obturator internus
- Obturator externus
- Gemellus inferior
- Gemellus superior
- Gluteus medius (posterior fibers)
- Gluteus maximus
- Biceps femoris (long head)
Weakness in the hip external rotators can cause a sensation of hip instability.
6. Hip Internal Rotators
The hip internal rotators perform the opposite action of the external rotators. They are responsible for rotating the knee and thigh inward.
The following muscles cause internal rotation at the hip:
- Gluteus medius (anterior fibers)
- Gluteus minimus
- Tensor fascia latae
- Adductor longus
- Adductor brevis
- Semimembranosus
- Semitendinosus
Properly working hip internal rotators are important for correct pelvic mobility and stability during the normal gait or walking cycle.
Nerves of the Hip
Nerves help to provide motor and/or sensory function throughout the body.
While there are many nerves that can be discussed around the hip, let’s take a look at a brief overview of the primary nerves that help to innervate the hip and can affect proper hip function.
1. Sciatic Nerve
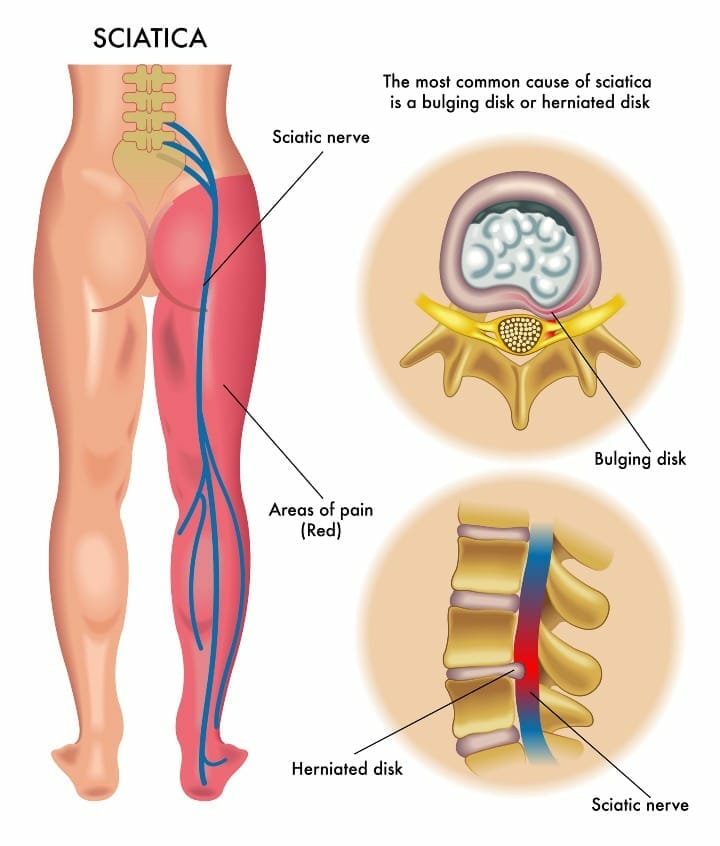
The sciatic nerve is the longest nerve in the body. It both innervates muscles and provides sensation.
It originates in the lower spine from L4-S3 and travels down the back of the leg, branching off into other various nerve segments.
Many will develop sciatica because of where the sciatic nerve runs under the piriformis muscle.
This can occur from a tight piriformis or any abnormal pressure on the muscle, subsequently causing excessive pressure over the sciatic nerve. This can cause pain and/or radiating symptoms down the back of the leg.
2. Femoral Nerve
The femoral nerve is also a very large nerve in the body. This nerve originates in the lumbar spine at the L2-4 nerve roots.
While the sciatic nerve innervates the back of the thigh, this nerve innervates the muscles and provides sensation in the front of the thigh.
As it travels down, it will split into an anterior and posterior division. The saphenous nerve will originate from the posterior division of the femoral nerve and innervate the leg from the knee and below.
3. Obturator Nerve
The obturator nerve, originating from L2-4, is located on the inner thigh or groin region.
It’s in this area that it provides both motor and sensory innervation to the inner thigh. This includes the inner thigh at both the hip and knee joints.
Lateral Femoral Cutaneous Nerve
The lateral femoral cutaneous nerve originates from L2-3.
This nerve provides sensory innervation to the anterior and lateral aspects of the thigh.
Blood Vessels of the Hip
Various blood vessels surround the hip and allow a proper supply of blood flow to the hip.
Vital hip blood vessels include the following:
- Femoral artery
- Lateral circumflex femoral arteries
- Medial circumflex femoral arteries
- Obturator artery
- Profunda femoris artery
- Retinacular arteries
A lack of proper blood supply, no matter the cause, can lead to the death of bone cells. This is known as avascular necrosis.
If not addressed immediately, avascular necrosis can lead to continuous bone breakdown and eventual collapse, significant weakness, and bony deformities within the hip joint, leading to pain and functional restrictions.
Conclusion
There you have it! Hip anatomy 101.
Remember, having a basic understanding of hip anatomy can be extremely beneficial to achieve and maintain optimal hip health, as well as address pain and injuries when they occur.
Knowledge is power!
Wondering What's Next?
Discover 11 Easy, At-Home “Stretch Exercises” for Stronger, Pain-Free Joints (click below)